
Since gaining independence in 2011, South Sudan has struggled to build a sustainable health system. All the efforts were severely disrupted when civil war broke out in 2013, devastating critical infrastructure and forcing dozens of medical centres to shut down, while also displacing millions of people.
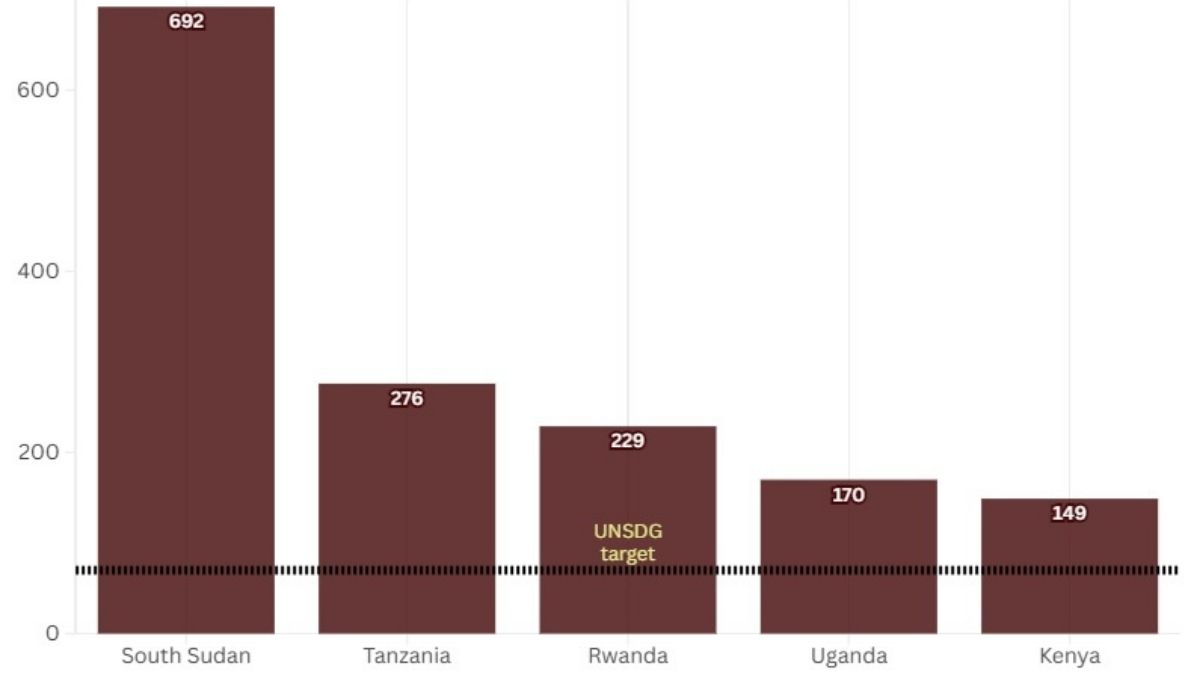
In conflict-affected regions such as Upper Nile and Jonglei, healthcare is scarce and often inaccessible. Even in the capital, Juba, access to quality maternal and child healthcare is a major challenge. According to assessments by the World Health Organization (WHO), South Sudan remains one of the world’s most dangerous places to give birth, as renewed violence has caused the collapse of health infrastructure, and chronic underinvestment continues to place mothers and children at extreme risk.
Conflict and Maternal Mortality
An analysis of maternal health indicators between 2015 and 2023 reveals how closely South Sudan’s maternal mortality trends mirror the country’s political instability. The period between 2015 and 2017, which marked the peak of the civil war, saw maternal mortality rise sharply. During this time, health facilities were destroyed or abandoned, supply chains for medicines collapsed, and thousands of trained health workers fled violence-affected areas.
Routine antenatal care became nearly impossible in many communities as displacement surged, and insecurity cut off access to basic services. Following the signing of Revitalised Transitional Government of National Unity (RTGoNU) in 2018, the peace agreement that ended South Sudan’s second civil war (2013–2018), maternal mortality began to decline. Between 2017 and 2023, the maternal mortality ratio fell significantly, reflecting improved security conditions, the gradual restoration of health services, and expanded humanitarian interventions.
As insecurity eased in many parts of the country, health facilities that had closed or ceased functioning during the 2013–2018 civil war were able to reopen and resume providing maternal health services.Improved security also enabled humanitarian organisations and development partners to expand investments in the health workforce.
After 2018, NGOs such as International Medical Corps scaled up structured midwifery training programmes, explicitly aiming to reduce maternal mortality by increasing the availability of skilled birth attendants. Together, the restoration of health services and the expansion of the maternal health workforce improved access to skilled care during pregnancy and childbirth, helping to contribute to the observed decline in maternal mortality, although other factors including continued donor support and broader health system investments.
However, progress has slowed in recent years, suggesting that the initial gains from restoring emergency services may have reached their limit.
Renewed Violence Threatening Fragile Health System
In December 2025, South Sudan experienced another escalation of violence involving the South Sudan People’s Defence Forces (SSPDF) and opposition forces linked to write full form here (SPLM-IO). Clashes in areas including Jonglei, Nasir, and Akobo have displaced thousands of civilians, many of whom now live in overcrowded and fragile conditions with limited access to healthcare, clean water, or sanitation.
“The war in Sudan, and the arriving of refugees and returnees have made the situation more precarious. The withdrawal of American support and the renewal of the war also make them more precarious. This is a crisis that may require more than just external intervention. It requires government intervention, for example, to increase health facilities. Health in the national budget is only 15-20%, which is very low,” said Frank*.
On 29 April 2026, Médecins Sans Frontières (MSF) announced that it was permanently closing its hospital in Lankien, Jonglei State, after the facility was bombed on 3 February 2026. The hospital had provided continuous medical care to the local population for more than three decades. In a statement, MSF said its facilities and staff had been affected by at least 12 attacks and violent incidents since the beginning of 2025. The violence has forced the closure of four hospitals in Ulang, Old Fangak, Akobo, and Lankien, leaving hundreds of thousands of people without access to essential medical services.
Fragile Infrastructure and Heavy External Dependence
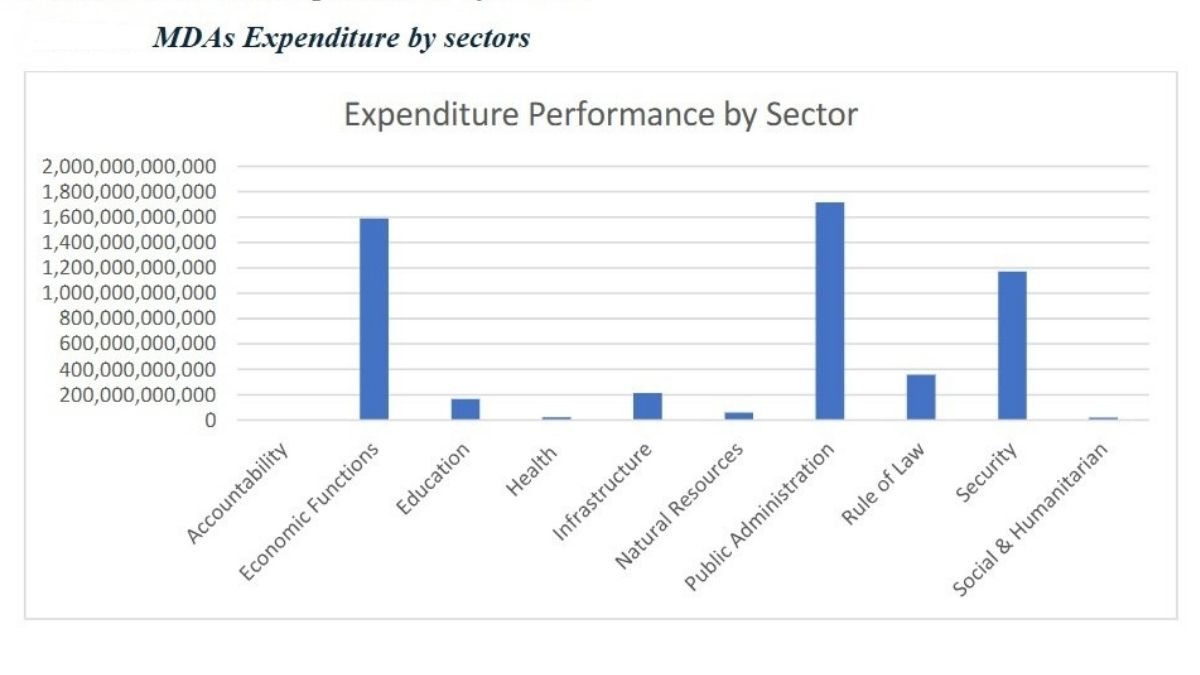
South Sudan’s health system is heavily dependent on international assistance. In many states, particularly Upper Nile and Jonglei, humanitarian agencies and NGO partners provide most basic health services. In their fiscal year 2024-2025 report, the South Sudan ministry of finance and planning data showed how low the health sector received from the overall budget of the country with the amount of SSP21,315,375,521.
According to Frank the system was originally designed around shared responsibility between government and international donors. “It is understood that the government is supposed to pay a portion and donors pay a portion. However, donors discovered that the government was unable to pay its share. This resulted in a funding deficit,” he said.
This dependence leaves the system vulnerable to funding cuts, logistical disruptions, and deteriorating security conditions. For example, the withdrawal of US embassy support from the National Health Laboratory has raised additional concerns about the country’s already limited capacity to detect and respond to disease outbreaks.
Rather than closing health centres, authorities responded by restructuring financial incentives for health workers. Frank added that a doctor who previously received USD600 per month will now receive USD400 per month under a new system expected to be implemented soon. This funding strain is reflected even at South Sudan’s largest public hospitals.
The Economic Crisis is Deepening the Healthcare Collapse
South Sudan’s worsening economic crisis has put further pressure on its already fragile healthcare system. Rising operational costs are being passed on directly to patients, and doctors at Juba Teaching Hospital say that this financial strain is affecting both diagnosis and treatment.
“We often see patients who cannot afford even a single test. Sometimes a patient can only cover part of the cost, forcing us to reduce the number of tests required and focus only on the most critical ones to reach a diagnosis,” said a resident physician.
These limitations also affect access to treatment itself, with some patients unable to purchase their full course of medication. This forces doctors to prioritise only the most essential drugs, and in more severe cases, financial barriers can delay or entirely prevent urgent surgical intervention.
“I have seen many fracture and trauma cases that should have gone directly to surgery, but patients returned home because they could not afford the tests, medication or the operation itself,” she added.
If Juba Teaching Hospital, the largest public referral hospital in the capital, is affected by shortages and affordability barriers, conditions are likely to be significantly worse in rural and conflict-affected regions, where many facilities depend on humanitarian organisations operating under shrinking budgets. While some organisations are working to sustain services outside Juba, health workers say these efforts are insufficient to meet national demand.
A Crisis That Must Not Be Ignored
South Sudan continues to battle some of the world’s deadliest preventable and treatable diseases, including malaria, cholera and typhoid. The country is also vulnerable to regional outbreaks such as Ebola due to its proximity to neighbouring countries Uganda and the Democratic Republic of Congo (DRC) where the epidemic first appeared in May 2026. On 15 April 2026, the Ministry of Health issued a statement about the Ebola outbreak in the DRC, despite the country’s limited disease surveillance capacity.
The maternal health crisis is closely linked to the wider collapse of the healthcare system. The risks that women face during pregnancy and childbirth do not stem from isolated failures in maternal care alone. These risks are instead a reflection of the deep-seated structural weaknesses plaguing the entire health sector, including chronic underfunding, deteriorating infrastructure, shortages of essential medicines, and an overreliance on external donors to sustain even the most basic services.
According to doctors, the crisis is not primarily due to a shortage of trained medical professionals, but rather to a lack of facilities, equipment, medicine and working conditions that would enable these professionals to stay in the country and provide effective care. The deteriorating conditions leave many with little choice but to seek opportunities elsewhere, which further weakens an already fragile system.
Until South Sudan treats healthcare as a national priority rather than an emergency sustained by external intervention and organisations, maternal deaths will continue to be a tragedy not only of childbirth, but also of a system that fails to provide basic necessities for mothers. Health workers warn that, without urgent increases in the public health budget, stronger investment in health infrastructure, better support for frontline medical personnel and sustained access to medicine and equipment, the system risks further collapse.
*A pseudonym has been used to protect the individual’s identity for safety and privacy.

500WM Columnist Dominica Amet Joseph Marco is a 26-year-old South Sudanese writer, freelance journalist and feminist/social activist who graduated from the faculty of law from the University of Bahri in 2018. She is one of many who had to flee war in Sudan to finally come and live in her homeland South Sudan. She has written and published articles, stories and poems since 2017. She has worked with and published articles in Aka’bar Alwatan Newspaper in Sudan, Almugif Newspaper in South Sudan, and several other Arabic websites.



{kind=link}